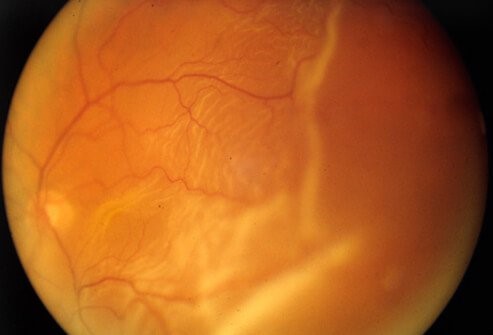
Dr. Cyres K Mehta’s International Eye Centre has made the biggest investment for our retina patients with the purchase of Zeiss Visucam 500 fundus camera, the best and most advanced non-mydriatic fundus camera for taking pictures of the retina
This camera has a few advantages
- You don’t have to dilate to take pictures of the retina
- It will do conventional Fluorescein angiography
- Zeiss optics are the best in the world
- It has Fundus autofluorescence(FAF) which can see the retina in great detail WITHOUT having to inject a dye into the patient. It can delineate membranes of macular degeneration and CSR lesions and is a great tool for noninvasive retina diagnostics
- It has MPOD which is only present in this device (Macular pigment density). Using MPOD we can actually track the progress of fry macular degeneration which was hitherto impossible.
The Zeiss Visucam 500 fundus camera helps in the detection and management of sight-threatening diseases like age-related macular degeneration, diabetic retinopathy, glaucoma, hypertensive retinopathy, cancer of the eye and other retinal diseases.